


Why Disease Control Fails in Conflict Zones like Gaza.
Polio, a public health crisis amid conflict and displacement.

Deformed legs, atrophied torsos, and the struggle to breathe. Those who survive polio are often left crippled by paralysis, facing a lifetime of disability and pain. Known historically as “infant paralysis,” poliomyelitis (polio) devastated communities for centuries before medical breakthroughs brought hope of eradication, with widespread vaccination campaigns curtailing poliovirus and its spread.
Back in July of this year, the World Health Organisation (WHO) raised alarms over a polio outbreak in Gaza. Despite risk assessments and attempts to prevent outbreaks, controlling disease in a conflict zone with crumbling sanitation services is nearly impossible. Even mass vaccination campaigns are hard to carry out when humanitarian workers face repeated delays and severe security risks. WHO noted that immunisation rates in Gaza and the West Bank were optimal before the conflict, with polio vaccine coverage reaching 99% in 2022. However, that figure has since dropped to 89%, leaving many children vulnerable and unprotected.
The most recent rollout relied on the localised pauses in fighting with around 560,000 children under 10 years of age vaccinated in the first round between 1-12 September in the Strip.

Each child has to receive 2 drops of oral vaccine in 2 rounds. The second must be administered 4 weeks after the first, therefore, the programme must be carried out quickly to prevent mutation and to break transmission. This latest outbreak is a prime case of this unfulfilled with a mutated variant starting an epidemic from an oral vaccine due to the weakened form of the virus in the vaccine evolving and being shed by those who have received it. To really understand what this means, let's break it down.
Emergence, Eradication, and then Re-emergence
Polio, short for poliomyelitis, is a highly infectious disease caused by the poliovirus, which belongs to the Enterovirus genus (intestine-related) within the Picornaviridae family (fancy words, not that exciting, it looks like a little ball, see below). There are three types of wild poliovirus (WPV): type 1 (WPV1), type 2 (WPV2), and type 3 (WPV3). WPV2 was declared eradicated in 2015, and WPV3 in 2019, leaving WPV1 endemic in only two countries: Afghanistan and Pakistan.
Polio is primarily transmitted via the faecal-oral route, although transmission can also occur through oral and nasal secretions. Once ingested, the virus multiplies, entering the bloodstream and, in some cases, the central nervous system (CNS). The virus specifically targets and destroys motor neurons in the anterior horn of the spinal cord and in severe cases, the virus can cause total paralysis within hours of infection. Poliomyelitis primarily affects children under the age of five, with paralysis occurring in approximately 1 in 200 infections. Of those paralysed, 5-10% die when their respiratory muscles become immobilised. Pretty scary considering up to 90% of those infected experience nothing or just mild symptoms and so the disease usually goes unrecognised = undetected spread.
Historically, the incidence of polio increased dramatically in the late 19th and early 20th centuries, leading to widespread epidemics in industrialised countries, even as other infectious diseases declined due to improved sanitation and hygiene. These paradoxical trends in polio transmission can be linked to the "hygiene hypothesis," where delayed exposure to the virus in cleaner environments resulted in more severe outcomes, as older children and adults are more likely to develop symptomatic polio.
The introduction of effective vaccines fundamentally altered the trajectory of polio control. In 1955, Jonas Salk developed the inactivated polio vaccine (IPV), an injectable vaccine containing killed poliovirus. IPV stimulates an immune response without the risk of infection from the vaccine. However, in 1962, Albert Sabin introduced the oral polio vaccine (OPV), which contains live, attenuated (weakened) virus strains of all three poliovirus serotypes. OPV, administered as oral drops, is cheaper to produce and easier to administer, making it a critical tool in global mass vaccination campaigns (big hooray for accessible and equitable healthcare).

OPV has several advantages in polio eradication efforts. It induces both humoural and mucosal (mucus/linings/you get the gist) immunity, basically meaning immunity throughout the body via the bloodstream plus the entry points like the mouth, nose, and intestines. Mucosal immunity in the intestines helps interrupt person-to-person transmission of the virus, an essential feature for achieving herd immunity (essentially when there are enough people immune to create a protective “shield” from getting infected around the whole community). However, a huge challenge as mentioned with OPV is the potential for vaccine-derived poliovirus (VDPV). So in rare cases, the attenuated (weakened) virus in the vaccine can mutate, regain neurovirulence, and circulate in populations with low immunisation coverage, leading to circulating vaccine-derived poliovirus (cVDPV) outbreaks. A valid concern in regions with disrupted health systems like Palestine.
IPV's role has become increasingly critical in countries with no active poliovirus transmission, whereas OPV continues to be an essential tool in regions where the virus still circulates or where health infrastructure is limited. In conflict zones like Gaza, the virus re-emerges as public health infrastructure crumbles and displacement creates unhygienic conditions.
War and WASH
Diseases don’t respect political situations or borders; they exploit environments where basic public health infrastructure has broken down. Mass displacement in conflict zones often results in overcrowded refugee camps or makeshift settlements, where access to clean water is scarce, sanitation is inadequate, and hygiene practices are difficult to maintain. These conditions create a high-risk environment for the spread of poliovirus.
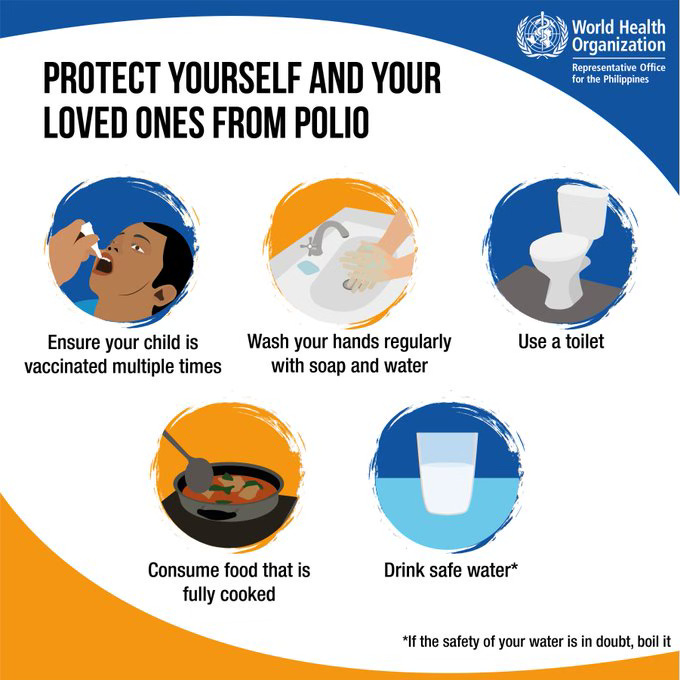
The role of WASH (Water, Sanitation, and Hygiene) in polio prevention is multifaceted:
access to clean water reduces the risk of consuming food or water contaminated with poliovirus.
effective sanitation — including the proper disposal of human waste — limits the environmental spread of the virus.
hygiene practices such as handwashing with soap interrupt the transmission of faecal-oral pathogens.
In fragile states like Gaza, WASH systems are often deliberately targeted during conflict, or they collapse due to neglect and lack of resources - even well-meaning public health interventions, such as vaccination campaigns, struggle to achieve their full potential without the support of functioning WASH systems. And it's hardly straightforward, security risks and logistical challenges can also delay or limit the reach of vaccination efforts.
In humanitarian emergencies, the risks for children multiply. Violence, displacement, and human rights violations become everyday threats. Children in conflict zones often face additional health burdens, such as malnutrition and weakened immune systems, which further increase their susceptibility to infections. Malnutrition impairs immune function, making it harder for the body to fight off viral infections, including polio. A stark reminder of the complexities of controlling infectious diseases in unstable settings.
Beyond Vaccines: Paralysis in Palestine
For centuries, polio immunity was naturally passed down from mothers who had survived the virus, transferring protection to their babies through pregnancy and breastfeeding. But with modern vaccinations, we now have the tools to protect every child from this debilitating disease.
Ensuring widespread vaccination in these regions is not just a matter of public health but also a moral imperative. It is a reflection of the complex interplay between multiple factors that shape health outcomes in fragile contexts. While the technical solutions for eradicating polio — vaccination campaigns and robust WASH systems — are well understood, implementing them in conflict-ridden environments requires addressing broader systemic issues.
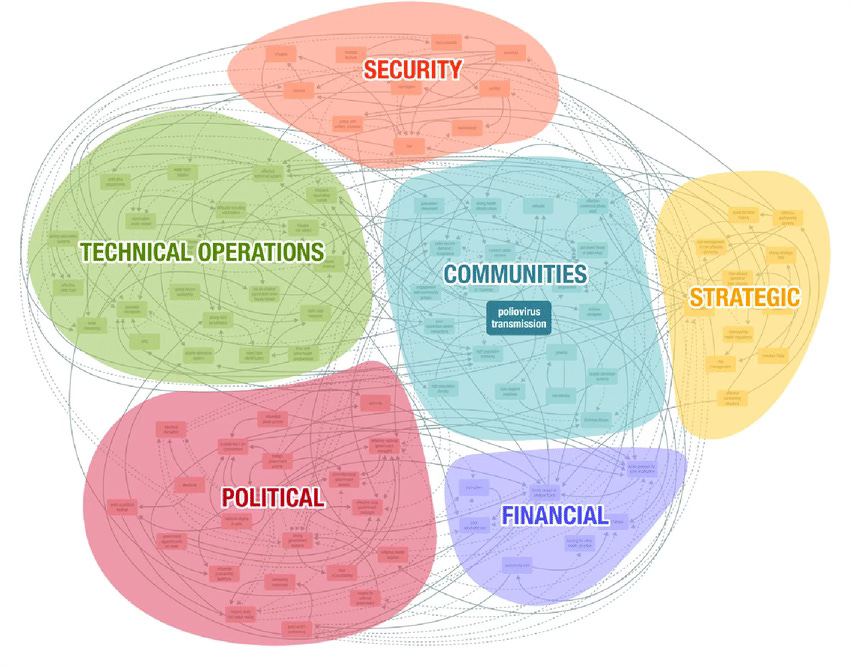
From an anthropological perspective, understanding how communities perceive health interventions, vaccines, and government or international aid is also paramount to cooperation. In many fragile contexts, mistrust of external actors, rooted in historical injustices and ongoing conflict, can lead to resistance to vaccination campaigns or other health interventions. In Gaza, years of political tension and isolation have fostered a deep-seated scepticism of both internal and external authorities.
Public health efforts are not simply medical challenges; they require coordinated efforts that integrate political diplomacy, community engagement, and social support systems to create lasting change. As the world edges closer to eradicating polio, the persistent threat in regions like Gaza reminds us that infectious diseases cannot be conquered by science alone.